
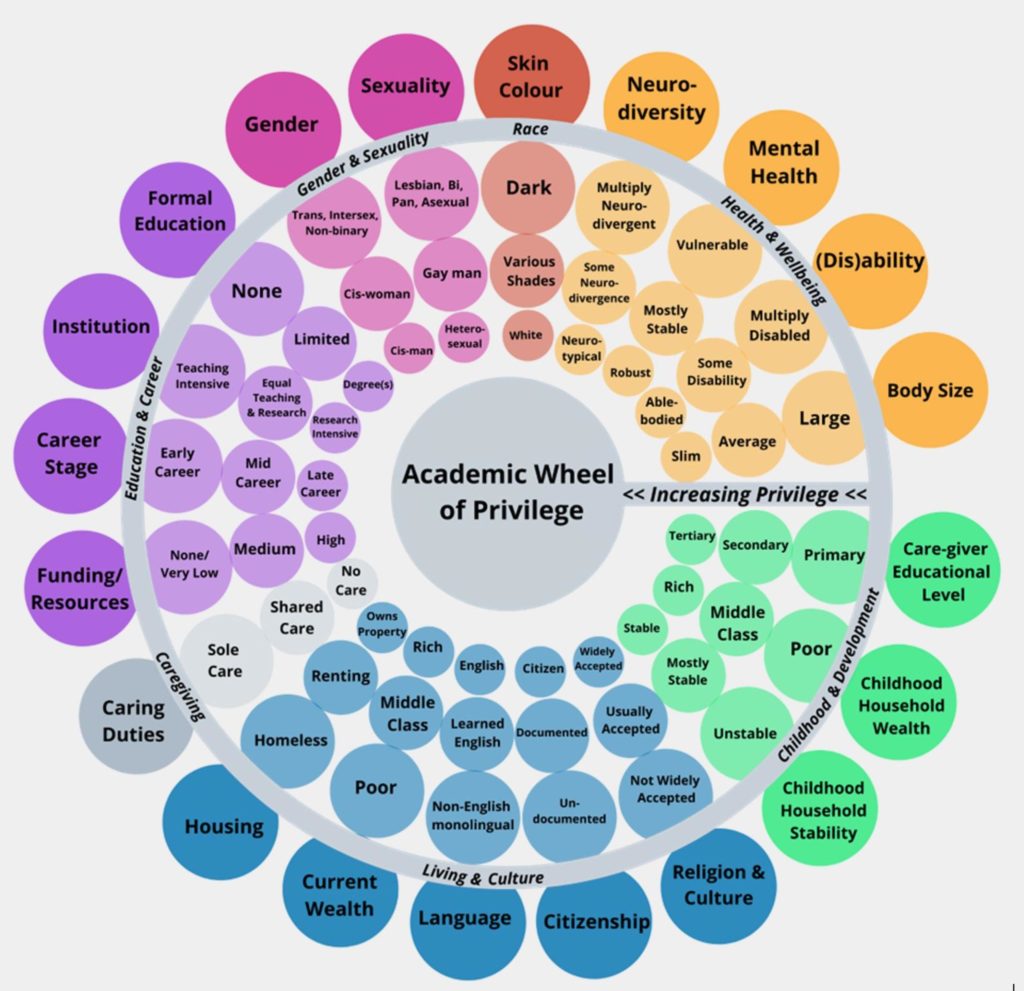
I think that privilege can be one of the most difficult things to explain to someone who either a) doesn’t understand it, b) has it, or c) fails to acknowledge that it exists. Often when I hear the word privilege, like many people, I usually assume that the context around it is from a racial standpoint. However, privilege exists in so many different dimensions. Privilege exists not only racially, but also based on gender, ability, socioeconomic status, age, sexual orientation, religion, citizenship, education level, and most associated with this class–health.
Understanding different forms of privilege is important to understanding how systems of inequality are perpetuated because privilege is one of the key mechanisms that perpetuates these systems. When certain individuals or groups have privilege based on certain identities that they possess, they have greater access to opportunities and resources that others (without those identities) do not. For example, studies have shown that prospective job employees with more ethnic-sounding names face hiring discrimination in comparison with their competitors with white-sounding names. This kind of discrimination leads to unequal variations in status, opportunity, and resources–that end up being key factors in the perpetuation of systemic inequality. However, learning about these inequalities and addressing them can help dismantle them to create a more equitable, just society.
Many of the inequalities that we have discussed in this class highlight an underlying trend of individuals with privilege–or lack thereof, and how this affects their lives. In the first week of class, we discussed the many pros and cons of the American healthcare system using readings from The Commonwealth Fund. Although there are pros–such as advanced care, technological innovation, and vast research–there are also many cons in the system that have detrimental effects to those that may not have some of the privileges that I listed above. Some of these cons include, but are not limited to, expensive costs of care, uneven investment in resources, lack of access, corruption, and disparities affecting marginalized groups.

The film that we watched in class, Remote Area Medical, was a powerful visualization of what some of the healthcare inequalities look like in this country. The film followed the nonprofit group that stages free clinics in Bristol, Tennessee that lacks access to basic health care. The film explained that Bristol has a bad drug problem and many of its citizens have done/do drugs, leading to various conditions such as lung cancer, bronchitis, lung disease. Many of the people living in Bristol are also blue collar workers that have no jobs or have low paying jobs with no insurance coverage.
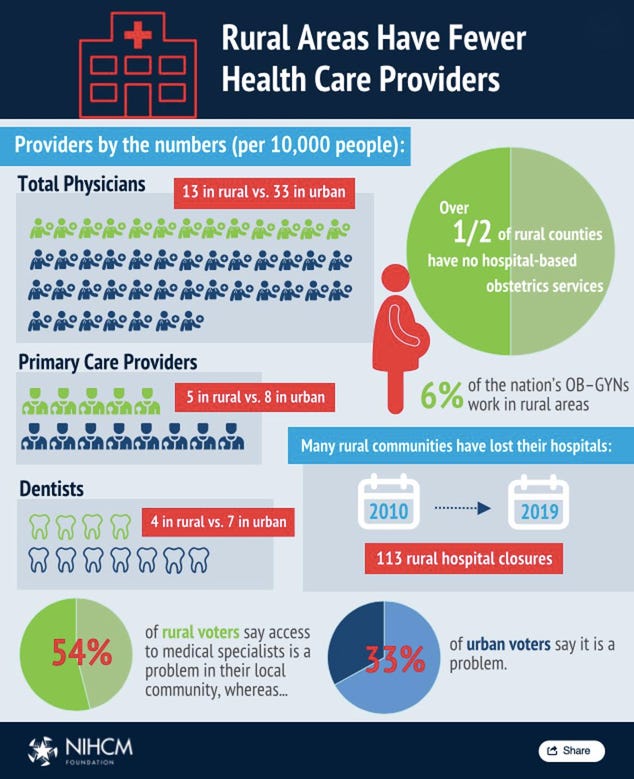
I think one of the biggest eye-opening moments for me from the film really was the way that privilege, in many different areas, was displayed. Because so many people in rural areas like Bristol do not have the resources or education to obtain college degrees, they are often forced to work in jobs with dangerous health implications such as jobs in the painting industry, automotive industry, and mining industry. Many of these jobs do not have medical benefits, which highlights one of the flaws in the American healthcare system, that there is no universal coverage.“Compared with the insured, uninsured individuals have a higher prevalence of chronic medical illness, greater physical morbidity, and higher mortality” (Washington, 2001). This would be an example of individuals lacking privilege from a socioeconomic standpoint that then affects their lives in other areas, such as health and education. While all of the patients in the film were white and do obtain privilege in their lives from their whiteness, and some may have privilege as it pertains to their physical ability or sexual orientation, they are all disadvantaged socioeconomically in one way or another. This demonstrates a key idea around privilege–that it is not one-dimensional.
For example, a white woman in America can experience sexism and not racism, while a Black woman can experience both. The white patients that were being treated in the film were disadvantaged academically and economically, but they were not discriminated against based on their race.
The socioeconomic statuses of the patients being treated by RAM significantly impacted their way of life and their access to quality medical care. Bristol, TN is over 90% white, so this racial makeup makes sense, however I could not help but wonder how the availability and accessibility of this free medical care could be different if Bristol was 90% Black. Would the clinic even exist? Would RAM try to make sure that the physicians that were volunteering represented the demographics of the people that they were serving? Would there have been racial bias within the diagnosis and treatment of certain conditions that are often racialized?
Understanding the intersectionality of privilege is critically important because it helps us to conceptualize that individual experiences that people have are constantly being shaped by their numerous identities, whether that be based on their race, gender, sexual orientation, socioeconomic status, or ability. These compounding identities intersect with one another that can either exacerbate or mitigate one’s privilege or lack thereof.
Sources
Blacksher, E. White Privilege, White Poverty: Reckoning with Class and Race in America. Moral and Social Challenges of Civic Learning. 25 February 2021. https://onlinelibrary.wiley.com/doi/full/10.1002/hast.1230.
University Libraries at Rider University. Privilege and Intersectionality. https://guides.rider.edu/privilege
United States Census Bureau. United States Census Bureau. 2022. https://www.census.gov/quickfacts/bristolcitytennessee
Bridges, K. Implicit Bias and Racial Disparities in Healthcare. American Bar Association. 2023. https://www.americanbar.org/groups/crsj/publications/human_rights_magazine_home/the-state-of-healthcare-in-the-united-states/racial-disparities-in-health-care/
UK Research Integrity Office. Academic Wheel of Privilege. 2023. https://ukrio.org/research-integrity-resources/equality-diversity-and-inclusion/academic-wheel-of-privilege/
Washington, D. Charting the path from lack of insurance to poor health outcomes. West J Med. July 2001. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1071459/#:~:text=Lack%20of%20health%20insurance%20is,it%20has%20significant%20health%20consequences.&text=Compared%20with%20the%20insured%2C%20uninsured,physical%20morbidity%2C%20and%20higher%20mortality.
Day, J. Rates of Uninsured Fall in Rural Counties, Remain Higher Than Urban Counties. United States Census Bureau. 9 April 2019. https://www.census.gov/library/stories/2019/04/health-insurance-rural-america.html
Roberts, N. Urbanization Leaves Rural America In A Health Care Crisis. Forbes. 25 October 2019. https://www.forbes.com/sites/nicolefisher/2019/10/25/urbanization-leaves-rural-america-in-a-health-care-crisis/?sh=36210e3d1b2a
Carlsson, M. Is It Your Foreign Name or Foreign Qualifications? An Experimental Study of Ethnic Discrimination in Hiring. ECONSTOR. November 2008. https://www.econstor.eu/bitstream/10419/35823/1/584702035.pdf