Do you experience deep, sharp pain in your groin? Or a feeling of “catching” or “popping” in your hip joint as you go about your daily activities? Is your range of motion you once had now severely limited? If so, you could be experiencing symptoms of a hip acetabular labrum tear, an ever-increasing problem in society that fortunately, has effective treatments.
What is the labrum?
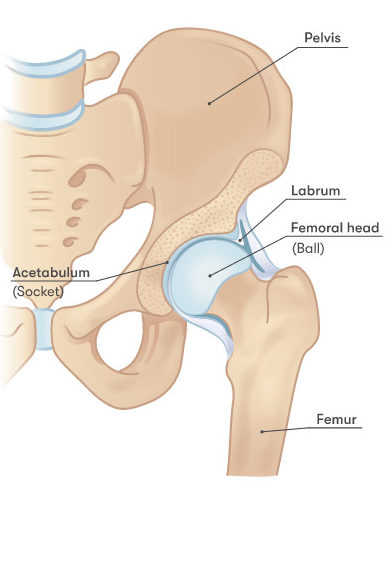
The acetabular labrum is a portion of tough cartilage that lines the rim of the acetabulum, or the “socket” of the “socket-and-ball” structure of the hip that allows us to move and rotate our leg in various directions. The main role of the labrum is to decrease friction between the bones, as well as protect the joint from strong impacts. Cartilage in the hip also stores synovial fluid, releasing it with motion to lubricate the joint similar to how a sponge releases water when squeezed.
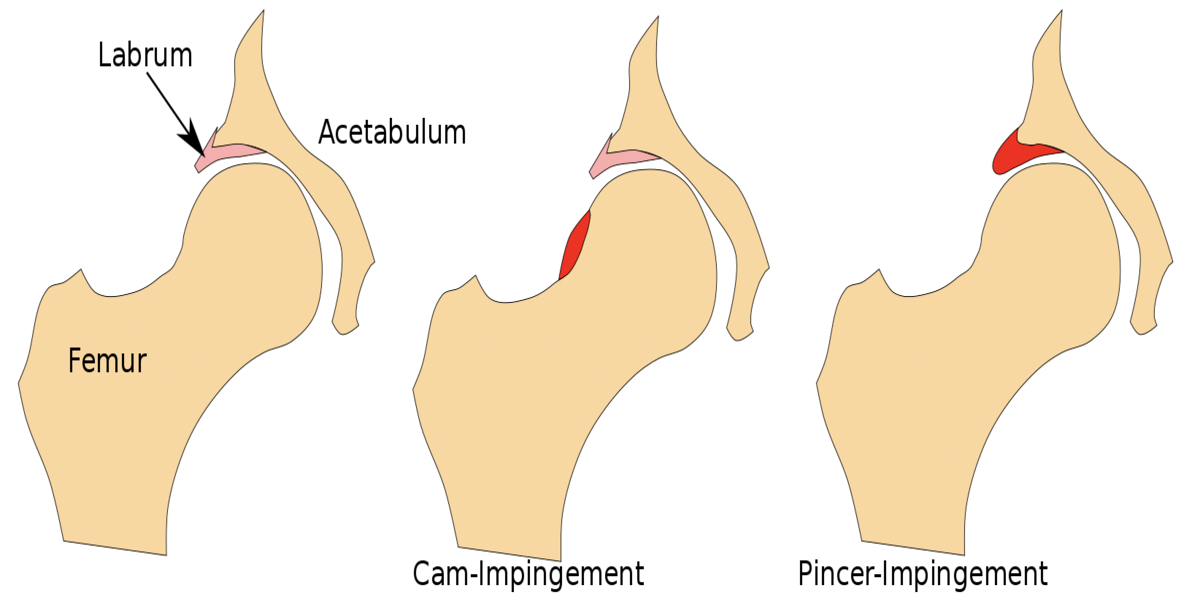
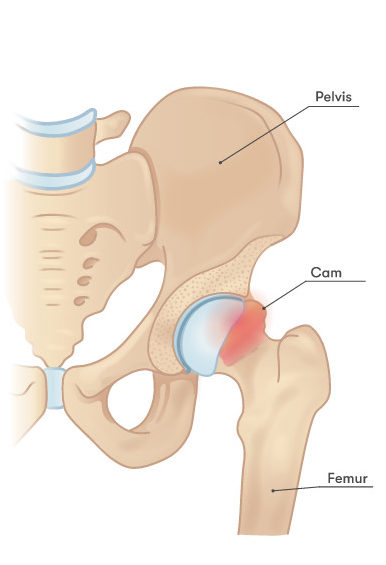
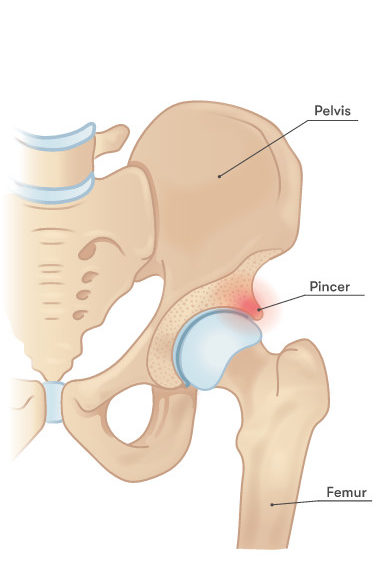
Labrums can be either traumatic or degenerative tears. Traumatic tears are typically a result of an accident, fall, or sports injury. Degenerative tears are chronic, and typically the result of femoroacetabular impingement (FAI). FAI is a condition in which there is abnormal bone growth around the joint, causing more friction and leading to eventual wear and tear of the labrum. There are two types of FAI: CAM and pincer, illustrated below. Surgeons can shave down the bony abnormality to recreate the normal shape.
The most common surgical techniques to repair labral tears in the hip include:
- Labral resection – smoothing or trimming down of frayed labral tissue is done to remove tissue causing pain
- Labral repair – the labrum is reattached to the acetabulum with suture anchors that hold it in place
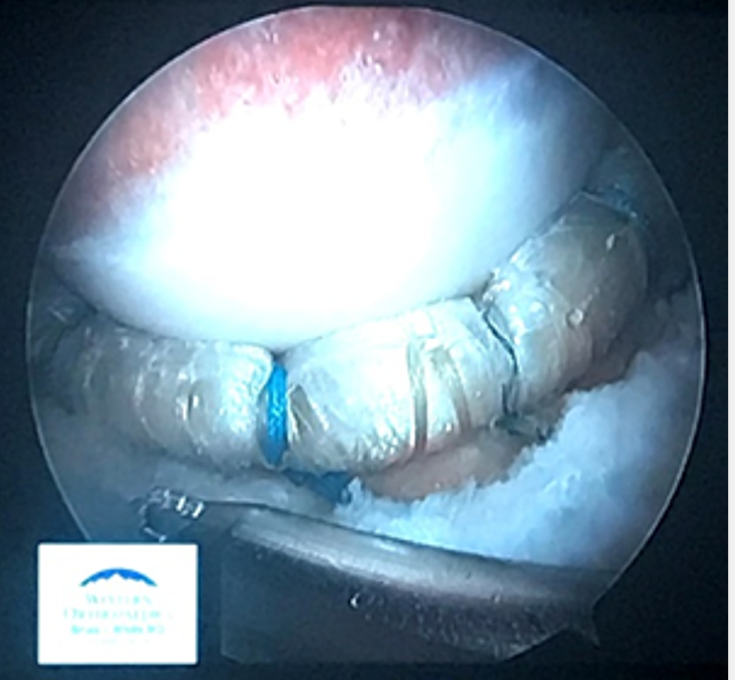
- Labral reconstruction – a piece of tissue is used to replace a damaged labrum when it is not repairable, the tissue is held in place with suture anchors along the acetabular rim
For a technique to be valid, the procedure must return the mechanical functionality of the hip joint to its intact state.
The Hip Fluid “Suction” Seal
During compressive loading experienced in walking, the suction seal of the hip pressurizes the synovial fluid stored within the cartilage. The suction seal is critical to the stability of the joint as well, as a negative pressure is created that restricts the femoral head’s motion due to unpredictable external forces.
One study investigated how various labral conditions affected the pressurization of the hip. Cadaver hip specimens with an age and gender distribution were secured in testing equipment in a position that modeled normal walking gait. Pressure sensors were placed in the capsule to measure fluid pressures as specimens were subjected to compressive forces. The results showed that a labral tear does significantly lower the intra-articular pressure of the hip, showing pressures that were 75% relative to the intact state. Labral resections reduce the pressurization even further below the values of a tear, while labral repairs and reconstructions both restore, and even improve, the fluid pressurization to the intact state.
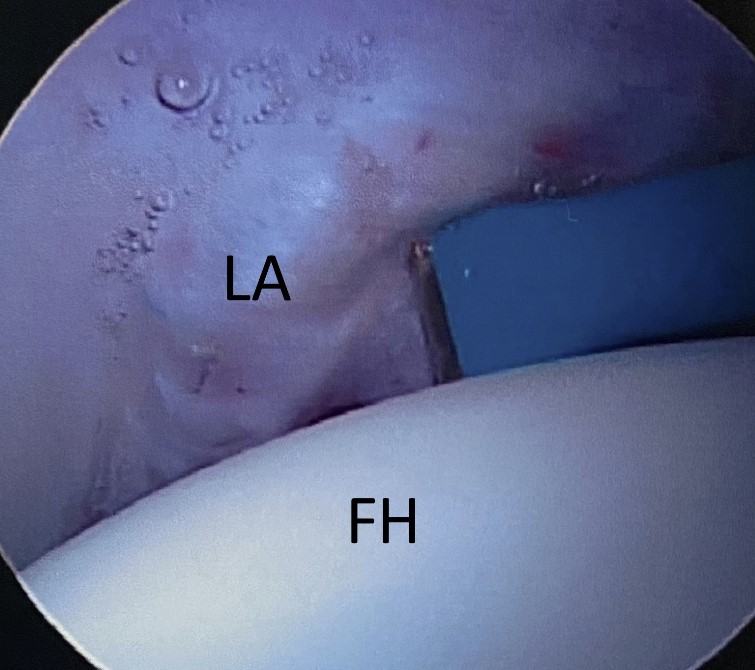
Another prominent issue related to the hip fluid seal is the increase in the number of revision hip arthroscopies due to capsulolabral adhesions. Adhesions are a build up of scar tissue that forms as the joint heals. They join to the surface of the labrum and the hip capsule, sticking to both and causing damage to their surfaces. In severe cases, these adhesions are so sticky that they can tether to the labrum and pull it away from the femoral head as pictured on the right, breaking the fluid seal and producing feelings of “giving way.” Dr. Marc Philippon, a leading hip preservationist, has developed both surgical and rehabilitative solutions to address this concern. In the surgical solution, the surgeon creates a “spacer” offset between the labrum and capsule to prevent adhesions from binding the two surfaces together and allow the labrum to maintain contact with the femoral head. The rehabilitation techniques utilize continuous passive motion to actively prevent the formation of adhesions, most notably circumduction. Low impact active range of motion exercises such as cycling or aquatic therapy is also encouraged to return blood flow to the joint.
Contact Area and Pressure
Since distributing load pressure and increasing the contact area to improve range of motion are two of the main functions of the labrum in protecting and stabilizing the femoral head, it was also important for researchers to investigate how contact area and pressure of labral conditions compared to the intact labral state. The measurements were taken in various degrees of extension and flexion to mimic stair climbing. It is optimal to have a greater contact area to distribute loads and increase range of motions, and a lower contact pressure to protect the bone against impact, so the labral resection was determined to be an insufficient technique once again since it did the opposite. Under the same criteria, it was determined that a reconstruction can return the labrum to more ideal conditions than the intact state.
Featured image modified from File:Femoral acetabular impingement FAI.svg under CC-BY-SA-4.0 via WikimediaCommons
{kind=link}